Developing a Religiously-Tailored Mammography Intervention for American Muslims
Why American Muslims?

Why Mammography?

Breast cancer is the second leading cause of cancer death among American women, and screening mammography is a proven method to reduce mortality from this cancer. In 2015 while 65.3% of U.S. women above 40 had a mammogram, lower rates were observed among racial and ethnic minorities. Muslim women have low rates of mammography.
Community surveys reveal:
- 37% of women (n=254) in the Chicago area had not obtained a mammogram in the last 2 years
- 42% of Arab women (n=365) from Detroit reported not having a mammogram every 1-2 years
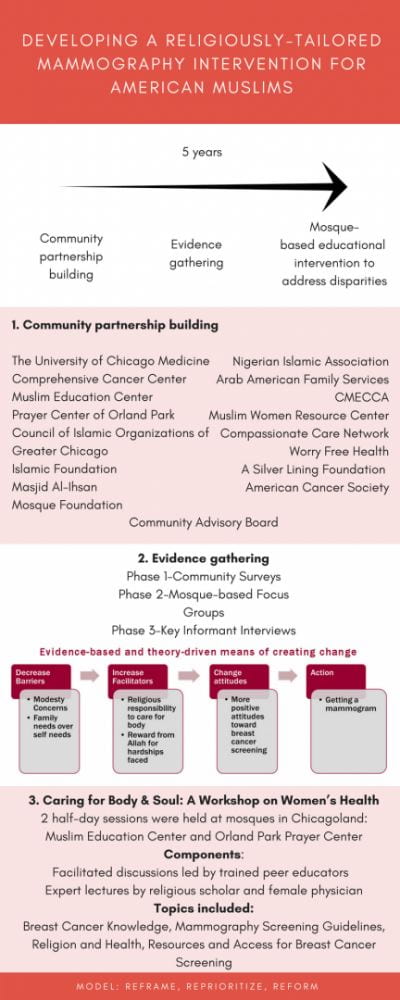
Developing Religiously Tailored, Evidence-Based Health Education for Muslim American Women

Community Partnership Building
- Council of Islamic Organizatons of Greater Chicago
- Muslim Women Resource Center
- Arab American Family Services
- Compassionate Care Network
Evidence Gathering
- Phase 1: Community Surveys
- Phase 2: Mosque-based Focus Groups
- Phase 3: Key Informant Interviews
Tailored Intervention Design and Deployment
- Caring for Body & Soul Workshops
- Group Education Manual – Replication Guide
Workshop Structure
- 2 half-day sessions were held at Muslim Education Center and Orland Park Prayer Center
- Peer-educators and guest lecturers, including a religious scholar and female physician, delivered didactics and facilitated discussion sessions on: breast cancer, mammography screening guidelines, religion and health, accessing resources for breast cancer screening

Methods for Addressing Barrier Beliefs: The 3R Model

Reframe: “switch train tracks”
- Keep the belief intact but change the way one thinks about it so it is consonant with the desired health behavior
- Normalizes the barrier belief
Reprioritize: “show them a better train”
- Introduce a new belief and create higher valence for it than the barrier belief
- Normalization of the barrier belief is optional
Reform: “breakdown the train carriage”
- Negate the barrier belief by demonstrating its faults by appealing to authority structures
Results
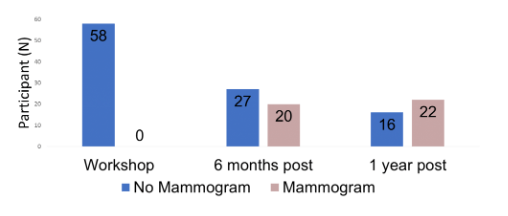
Of the 58 participants in workshop:
- Demographics 35% of participants were of Arab decent
- 52% of participants were of South Asian decent
- 37% of participants annual income was below poverty level

- Mammography
- 27/58 participants had NOT had mammogram in the past 2 years.
- 29/58 participants had NEVER had a mammogram
Within 1 year after this workshop:
- 22 participants (38%) had received a mammogram within one year of the classes
Project Outputs
Academic Papers
- Changing Mammography-Related Beliefs Among American Muslim Women: Findings from a Religiously-Tailored Mosque-Based Intervention.
-
The Development and Validation of a Modesty Measure for Diverse Muslim Populations.
-
Adapting a religious health fatalism measure for use in Muslim populations.
-
Acceptability of Friday Sermons as a Modality for Health Promotion and Education.
Media Highlights
Replication Toolkit
Replication Guide
Community members who are interested in replicating these workshops in your mosque can use our Replication Toolkit as a guide to learn more about the study design and logistical plannings to coordinate the workshops.
Friday Sermons
We wanted to assess the acceptability and feasibility of using sermons for health promotion in American Muslim mosque communities by deploying a tailored sermon in two mosque communities. Our study demonstrates that theologically-framed health messaging is acceptable within sermons in American Muslim mosque communities and underscores the potential utility of mosque sermons for health education programs and for health behavior interventions in American mosques. Below are sample sermons delivered in our study.

Memorial Sloan Kettering Cancer Center
Dr. Aasim Padela is speaking at Immigrant Health and Cancer Disparities Service on addressing mammography disparities among Muslim American women.

Mosque Partners
Orland Park Prayer Center (OPPC)

Mosque Partners
Muslim Education Center (MEC)
Developing Religiously Tailored Intervention
Building Community Partnerships, Evidence Gathering, and Pilot Testing.
The ‘3R Model’

3R Model: Reframe, Reprioritize, and Reform.
Supported by:

Community Advisory Board
-
Fatema Mirza*
-
Nancy Romanchek*
-
Tabassum Haleem
-
Masood Iqbal
-
Luma Mahairi
-
Beenish Manzoor
-
MahRukh Mian
-
Zakiyah Moton
-
Lynn Salahi
-
Kifah Shukair
-
Lila Zegar
*Indicate members that were also Peer Educators