
Auto Text: “Insert Breast Lumpectomy”
One of the most important aspects of grossing breast specimens is to correlate what you see grossly to what was seen radiographically. Prior to grossing, always check (1) radiology reports and (2) Epic records.
Specimen orientation and education: Seek guidance from a PA at triage and grossing (and potentially the triager), BEFORE the specimen is manipulated. Present and discuss a course of action for overall specimen assessment, gross description, and block submission.
Triage
- All breast resections for tumor must be triaged and placed in formalin within an hour of receipt, in order to minimize cold ischemic time and preserve antigenicity for receptor status (per CAP guidelines). Therefore, breasts cannot sit in the OR fridge overnight, and must be triaged even if they arrive late in the day. If a breast case is going late in the OR (i.e. past 7pm), the gross room resident, PAs, and if necessary, LMROC, should discuss timely triage of the specimen.
- If you receive a Breast with radioactive seeds, please consult a PA and read procedure UCMC 1145 in MediaLab (Handling Radioactive Specimens in the Gross Pathology Laboratory).
- Trace the specimen on the grid, noting where sutures and wires are located.
- Verify that the orientation and laterality on the requisition matches the container label and the actual specimen. If there are discrepancies with the orientation or laterality, page and speak to the attending pathologist and/or surgeon before proceeding.
- Weigh.
- Measure:
- medial to lateral
- superior to inferior
- anterior to posterior

- Remove all vascular clips before inking.
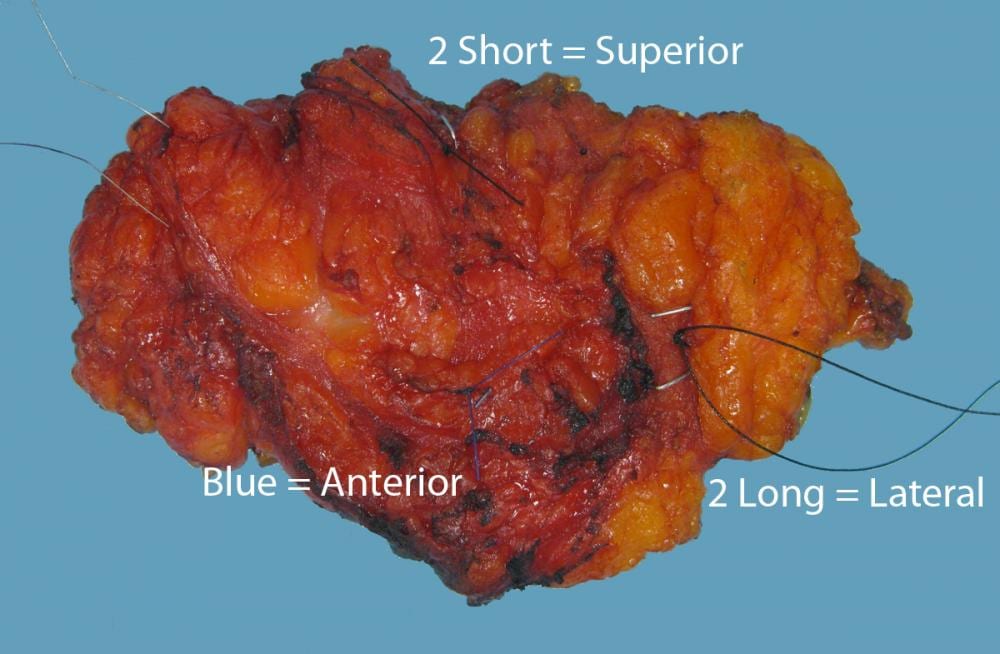
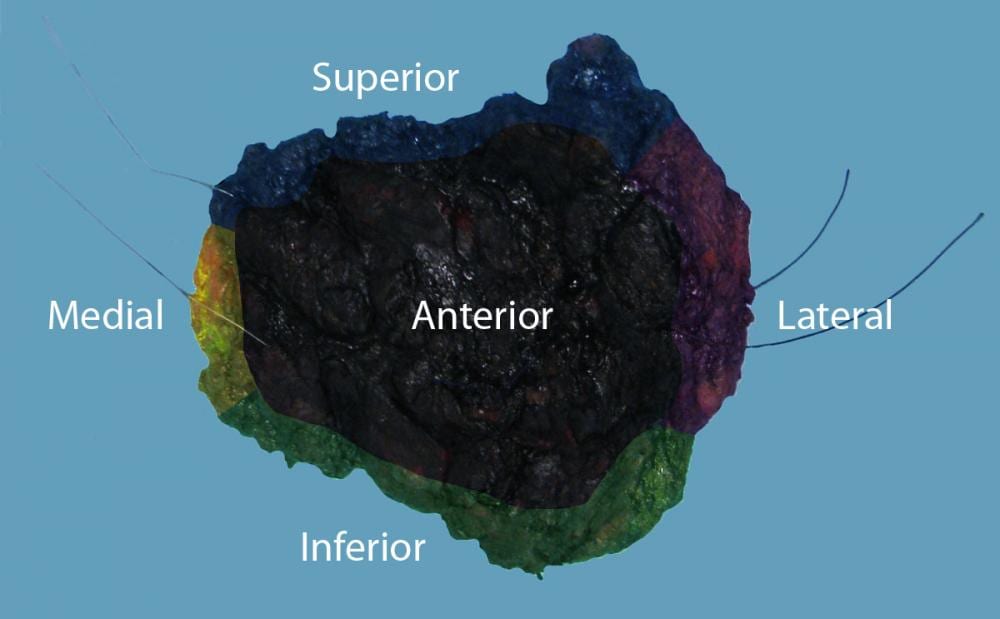
- Ink as follows (If you deviate from this convention, please CLEARLY indicate):
- First ink:
- medial – yellow (area size of a quarter)
- lateral – violet (area size of a quarter)
- Then ink:
- anterior – black
- posterior – red
- superior – blue
- inferior – green
- Dry off excess ink with paper towels. Apply vinegar to aid in ink adherence to tissue.


- Scan all lumpectomies INTACT with the Faxitron. Save image of clip(s) under the accession number. Contact the attending pathologist if the indicated number of clips (according to EPIC records) are not identified!
- Serially section the specimen from medial versus lateral or lateral to medial (start from the side with the area of interest/lesion). Section towards the tip of the wire or remove the wire before sectioning. Note where the wire is entering/terminating.
- Lay out the slices in sequential order on a paper towel. Do not keep intact “bookends” as in a mastectomy.
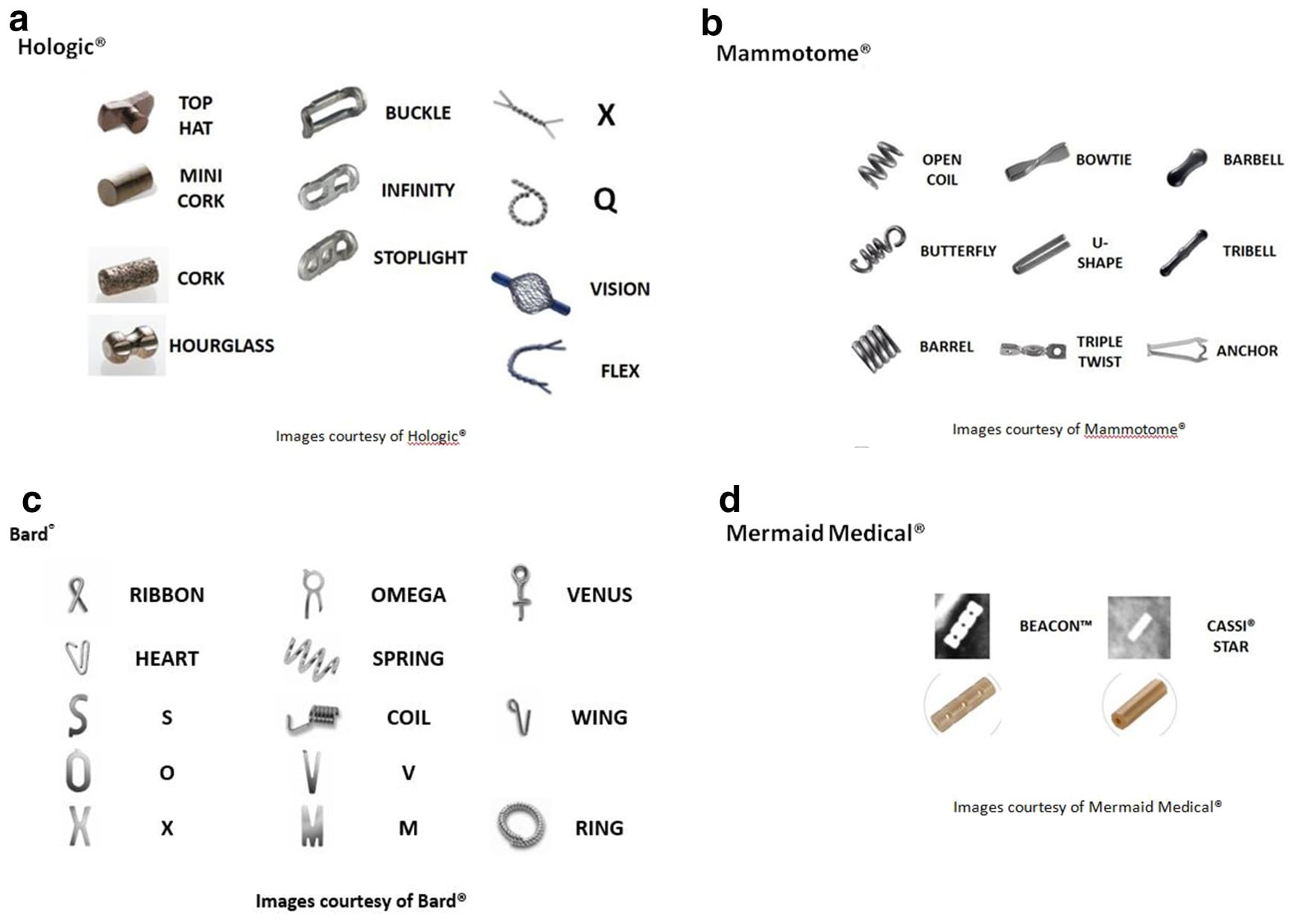
- Look for clip(s) and biopsy site change(s). See below for images of various clips. Faxitron the specimen if the clip(s) is not grossly identified. Contact the attending pathologist if the clip(s) identified before sectioning is no longer there!
- Do not remove clips from the specimen. Designate the slice number each clip is in. Mark the location of the clip(s) in the specimen with a pin. If the clip(s) fell out during sectioning, be sure to note that on the triage sheet.

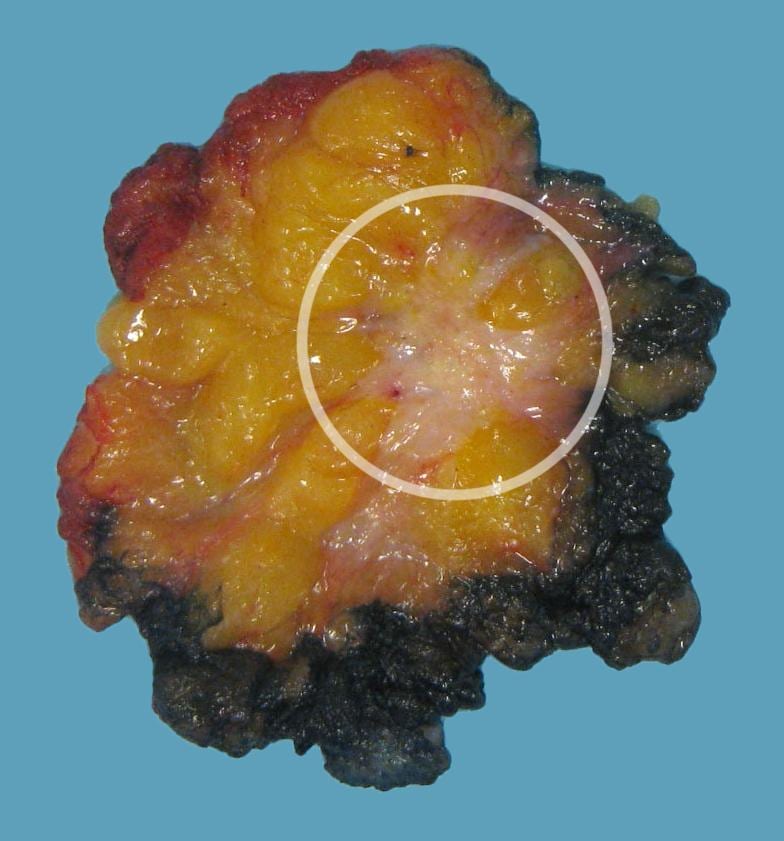
- Identify and carefully measure the lesion(s), designating medial to lateral, superior to inferior, anterior to posterior dimensions. Note in which slices lesion is located.

- Measure distance of lesion(s) to nearest margins.
- For multiple lesions, note spatial relation (i.e. lesion #1 is superior to lesion #2), distance between lesions, and total span of lesional tissue.
- Wrap the slices in a paper towel. Do not use rubber bands – this will distort the slices!
- Fix in formalin.
- Note the time the specimen is placed in formalin.
- Ensure that the specimen is in a container in which the volume of formalin is 10-times the volume of the tissue.



modified from Shah AD, et al. Clin Imaging. 2018 Nov-Dec;52:123-136.
Gross
- For each case, consult with a PA and/or the person who triaged the specimen.
- Serially section medial and lateral margins (perpendicular to margin) and submit entirely, perpendicularly, in designated cassettes.
- If present, take representative section of skin, noting which slice.
- Tumor submission – All cases are unique and this manual is only a guide. General guidelines are:
- Breast specimens that are listed as an excisional biopsy or are <5 cm in greatest dimension should be entirely submitted.
- For lesions <2 cm, submit entirely.
- For lesions >2 cm, submit 2 representative sections per cm of lesion.
- For post-treatment tumor beds, submit entirely if <2 cm. If >2 cm, submit 2 representative sections per cm of tumor bed.
- All lesions, discrete or ill-defined, should have one flanking section submitted on both sides of the greatest dimension measurement or extent of radiographic abnormality.
- Indicate which blocks contain the closest margins and confirm that those sections have appropriate and discernable ink.
- For ALL breast cases, dictate the following: Tissue fixed for at least 6 hours in 10% NBF and no more than 72 hours. (Auto Text: “Insert Breast Fixation”)
- Cassettes should be no more than 50% full of tissue with a maximum thickness of 2-3 mm.
