
Composite oral resections (including mandible, maxilla, palate, ear, temporal bone) require proper orientation and can be complex. CONSULT an attending at the time of triage. Always take gross photographs (BOTH intact and after sectioning).
Remember: For any tumor adjacent to / involving bone, if any part of the tumor is SOFT and does not NEED decalcification, please isolate 1-2 sections and submit as non-decalcified tumor. Then proceed with fixation and decalcification as necessary for the remainder of the case. Consider submitting a section in EDTA if the entire tissue requires decalcification (consult an attending).
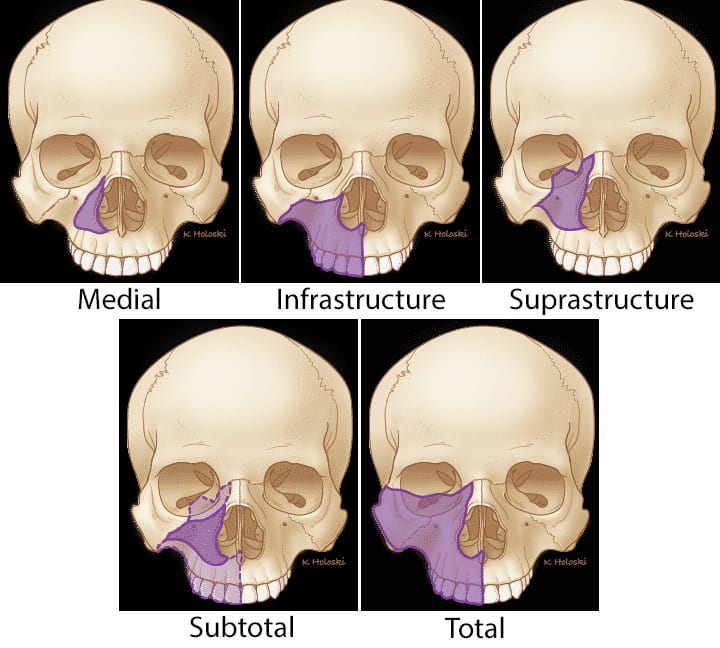
Types of Maxillectomies
- Medial maxillectomy: the part of the maxilla that is next to the nose is removed, but the eye and the hard palate are preserved.
- Infrastructure maxillectomy: the hard palate and lower portion of the maxilla with teeth are removed. It does not require the removal of the orbital floor.
- Suprastructure maxillectomy: the upper portion of the maxilla and orbital floor are removed, but the hard palate is left intact. The orbit may be removed or left in place.
- Subtotal maxillectomy: removes only part of the maxilla using some variation of the above procedures.
- Total maxillectomy: the entire maxilla as well as the hard palate and orbital floor are removed. When the orbit is removed during this surgery, it is termed total maxillectomy with orbital exenteration.
https://thancguide.org/cancer-basics/treatments/surgery/ablative/maxillectomy/
Triage
- Orient specimen, noting laterality, anterior-posterior, superior-inferior, and medial-lateral.
- Photograph fresh specimen (prior to sectioning) in all planes that are helpful for visualization.
- Measure specimen in 3D (A-P, S-I, M-L). If applicable, separately measure bone versus attached large pieces of soft tissue / skin.
- Ink Margins: Think before you ink and discuss with attending!
- Plan out your grossing strategy before inking. You can use different colors if it will help your later prosection (such as medial and lateral sides different colors).
- Ink peripheral soft tissue margins.
- If a bone margin will be taken en face, it does not need to be inked. If a bone margin will be taken radially, ink the cut surface (looks like marrow surrounded by cortex).
- NOTE: The outer surface of thick bony cortex / subperiosteum does not usually need to be be inked, as it often rubs off and can be cumbersome.
- If specimen is small with delicate bone, fix in formalin overnight. If large, you might want to section prior to fixation, to allow better penetration of formalin. DISCUSS WITH ATTENDING!

Gross
- Margins to consider include:
- Mucosal (for tumors that originate or spread along mucosa, such as SCC or melanoma).
- Soft tissue.
- Bone (cut surfaces).
- Always discuss your approach to grossing with an attending.
- Specimens can usually be sectioned in one direction (perpendicular to long axis).
- Photograph cut sections prior to decalcification.
- In order to facilitate decalcification, we recommend you cut your sections with a bone saw FIRST, and then decalcify thin sections. You can always thin down your sections after initial decalcification if they are too thick.
- For SMALL, DELICATE specimens, consider complete decalcification followed by sectioning with a long blade. ALWAYS consult an attending FIRST if this is your plan.
- Teeth will decalcify, but fillings or other foreign materials will NOT. If these materials are present, do NOT submit for histology.
- Always dictate which blocks were decalcified (or if entire specimen).
New NAC 06-23-2020
