
Contact Dr. Pytel before beginning any eye enucleation for tumor.
Auto Text: “Insert eye enucleation”
Triage
- Identify anatomic landmarks on the anterior and posterior aspect to help orient the specimen. If you have questions about orientation, please speak to one of the pathologists’ assistants or Dr. Pytel.
- Anterior
- Cornea is slightly longer horizontally/medial to lateral
- Posterior
- Long posterior ciliary arteries enter at posterior aspect of globe, adjacent to optic nerve and run along the medial and lateral aspects, deep to the sclera
- Vortex veins exit the sclera at the posterior aspect of the globe, but are found superior and inferior to the optic nerve
- Superior oblique muscle is more tendinous, and inserts on the superolateral aspect of the posterior globe, under the superior rectus muscle
- Inferior oblique muscle is more muscular, and inserts on the lateral aspect of the posterior globe, under the lateral rectus muscle
- Anterior
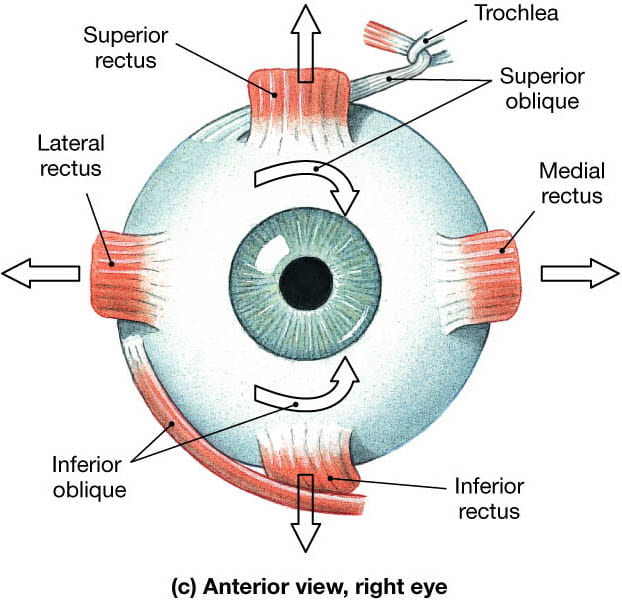

Image courtesy of: E. Heidi Cheek, MHS, PA(ASCP) and Diva R. Salomao, MD, Department of Pathology, Mayo Clinic, Rochester, Minnesota, USA; used with permission.

© 2019 American Academy of Ophthalmology.
- Take gross photographs of the anterior and posterior aspect of the globe
- Measure the globe in 3 dimensions (superior to inferior, medial to lateral, anterior to posterior)
- Measure the optic nerve length and diameter
- Measure the cornea in 2 dimensions
- Medial to lateral slightly longer than superior to inferior
- Measure the pupil in diameter
- Describe the cornea
- Opaque versus clear versus other
- Describe the color of the iris
- Describe the quality of the sclera
- Intact, disrupted, white, red, etc.
- Ink the medial rectus muscle black, and the lateral rectus muscle blue
- Shave the optic nerve margin and submit en face
- Place the globe in formalin and allow to fix for 24-48 hours
Gross
- Wash in running tap water for 5-15 minutes before sectioning
- Check EPIC to see if there are any notes on where the tumor is found (nasal versus temporal, superior versus inferior)
- Use the dissecting microscope to examine for any shadows on the sclera, as this may represent the tumor
- In addition, the Faxitron may be used to also try and show the location of the tumor
- Depending on the location of the tumor, the globe will need to be sectioned either horizontally, vertically or obliquely to ensure that the tumor is in the same plane as the optic nerve and pupil
- Using a short trim blade, take your first section 0.5 cm central to the limbus (where the sclera meets the cornea). This section is referred to as a calotte, or simply, a cap.

© 2017 College of American Pathologists.
- After taking your first section, examine the eye contents (preferably with a dissecting microscope).
- Measure/describe:
- Size, shape, color, consistency of tumor
- Location of tumor
- Superonasal quadrant, inferotemporal quadrant, anterior chamber, clock position, etc.
- Where tumor arises
- Retinoblastoma = retina
- Melanoma = choroid or ciliary body
- Whether it involves cornea, iris, lens, anterior chamber, ciliary body, vitreous chamber, retina, choroid, sclera
- Any extrascleral extension?
- Distance to optic nerve margin

Image courtesy of: E. Heidi Cheek, MHS, PA(ASCP) and Diva R. Salomao, MD, Department of Pathology, Mayo Clinic, Rochester, Minnesota, USA; used with permission.
- Using the short trim blade, make your second cut by sectioning through the limbus opposite of your first cut (i.e. if your first cut was through the superior limbus, the second will be through the inferior limbus)
- You should end up with two caps and a central section
- Place the central section in a mega cassette found in the tissue banking area
- Write the case number, MRN and patient’s last name using tissue-tek pencil
- Serially section each cap perpendicular to the cornea and entirely submit separately
