
Auto text: “Insert Lung Resection”
Prior to grossing the specimen, review any prior known pathology and recent chest imaging. Note the number of lesions, their size, location and relationship (if multiple). Make sure that gross correlates are found for all mass lesions detected radiographically. Ask a PA or Attending if you require assistance finding lesions.
Triage
- Weigh and measure (3D).
- Photograph the external surface.
- Take cross sections of the bronchial and vascular margins. If more than one lobe is present, make sure you designate the upper, middle, or lower lobe bronchial margins. Save in cassettes in the specimen container.
- If there is palpable tumor, ink the overlying pleura. Note pleural puckering in image:

- If the case is suspected tuberculosis, inflate the lung under the hood and fix overnight (24 hours): Using large syringe, inject formalin into bronchial tree.
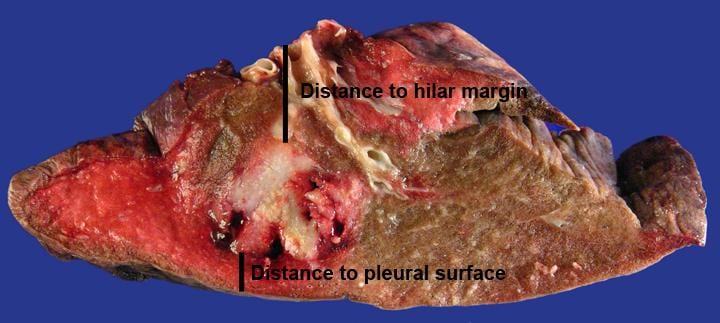
- If the case is for a hilar tumor, it may be cut open in the fresh state: Open the lung by inserting two probes down divergent airways, then cutting with a long knife along the probes. This method has the advantage of demonstrating the relationship of tumor to bronchial margin and pleural surface simultaneously (see image). Serially section the remainder, parallel to this cut.

- If the tumor is peripheral, thin serial sections of the lung is appropriate.
- Obtain tumor dimensions and general location within the lung, including proximity to the pleura, proximity to the nearest surgical margin of resection (if applicable), and distance to the bronchial margin.
- Photograph the cut section(s).
- Submerge in formalin and fix overnight.

Gross
- Lymph node dissection: Dissect off lymph nodes and keep track of how many nodes are submitted within each area (hilar, lobar/interlobar, segmental). Submit all the lymph nodes that you find according to these three areas:
- hilar: at mainstem right and left bronchi within hilar fat
- lobar/interlobar: at or between lobar bronchi (remember 2 on left, 3 on right)
- segmental: after first branch of lobar bronchus

- If the greatest dimension of the tumor is less than or equal to 1 cm, submit the whole tumor. If the greatest dimension is larger than 1 cm, submit representative sections, at least 3 and no more than 6 sections (including frozen section, if performed). Submit sections demonstrating relationships with adjacent uninvolved parenchyma and resection margin(s)/pleura. (NOTE: Tumor may have been banked prior to grossing – these measurements are of the fresh size before removal of tumor for tissue bank).
- Document involvement (if present) of parietal pleura, chest wall, pericardium, diaphragm.
- Examine the remainder of lung for satellite nodules or parenchymal abnormalities.
- Satellite nodules: Are common and are often found by careful palpation of thin slices. If present, measure their distance to the index lesion, to closest pleura, and to closest bronchial margin. Submit entirely.
- Parenchymal consolidation or discoloring (pale, yellow or white, dusky): Describe and submit 2 representative sections.
- No additional gross abnormalities: Submit 1 representative section of uninvolved lung.
- Don’t forget to submit previously-sampled lymph nodes and bronchial & vascular margins.

Updated SRR 12/11/24
