
Auto text: “Insert Penis”
Triage
- The majority of these resections are for invasive squamous cell carcinoma.
- Due to the rare nature of these resections, show all intact specimens to an attending pathologist.
- Take gross photographs – intact and after sectioning.
- Measure the overall length and diameter, as well as the foreskin (if applicable).
- Measure grossly identifiable tumor.
- Ink right and left sides differentially and fix overnight.
Gross
- Cut the glans and shaft longitudinally (sagittally) through the center. This section should cut the urethra and corpus spongiosum into right and left halves.
- Make note of the size, location, color, growth pattern (fungating, papillary, ulcerated, verrucous), consistency, margin involvement or distance from proximal resection margin.
- Document involvement (if any) of the foreskin, frenulum, glans, meatus, subepithelial connective tissue, corpus spongiosum, corpora cavernosa, urethra, prostate, or other structures.
- Sections should include:
- Proximal margin (skin, corpora, and urethra).
- Two to four cassettes of tumor showing deepest invasion and relationship to other structures.
- Additional lesions.
- Representative uninvolved penis.
Anatomy:
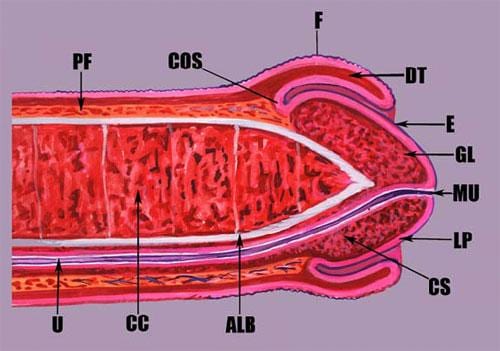
Midsagittal section showing (clockwise) Buck’s (penile) fascia (PF), coronal sulcus (COS), foreskin (F), dartos (DT), epithelium (E), glans (GL), urethral meatus (MU), lamina propria (LP), coronal sulcus (CS), tunica albuginea (ALB), corpus cavernosum (CC), ventral urethra (U) and surrounding corpus spongiosum. (from https://documents.cap.org/protocols/cp-penis-17protocol-4010.pdf)
