
Auto Text: “Insert Colon Tumor” or “Insert Rectal Tumor”
A variety of operations are performed in the treatment of colonic and rectal adenocarcinomas:
- transanal mucosal resection, performed for superficial rectal tumors, consists of tumor and surrounding mucosa +/- muscularis
- right hemicolectomy, with terminal ileum as proximal margin
- abdominal perineal resection (APR), performed for low rectal tumors, with anal skin as distal margin
- low anterior resection (LAR), performed to save sphincter function and avoid a colostomy, with tumor quite close to the distal resection margin
Notes Regarding Gross Exam of RECTAL Tumors
- ALWAYS photograph the mesorectal envelope (whether complete or incomplete).
- *Per Dr. Hart: Take a total of 4 images before opening: anterior, posterior, and each lateral view*.


- Almost all rectal cancers receive pre-operative chemoradiation treatment. This means that at the time of surgery only an ulcer or a scar (tumor bed) may be evident, indicating the site of prior tumor. If only a tumor bed is evident, the entire lesion (ulcer, scar) should be submitted for histologic examination. However, if residual tumor is grossly evident, only representative sections focusing on the area of deepest invasion are needed.
- It is critical that a measurement of the distance from the deepest extent of the tumor/ulcer to the inked radial margin be included in the gross description.
- All of the perirectal lymph nodes should be submitted for histologic examination. At least 14 lymph nodes is required per surgical and pathology guidelines. If you cannot find adequate lymph nodes, ASK A PA for help. If less than that number are identified grossly, then at least 10 ADDITIONAL cassettes of perirectal fat should be submitted.


Triage
- For transanal mucosal resections, identify any orienting sutures and ink deep and lateral margins. Measure in 3D. Pin on wax and fix in formalin.
- For large resections, identify the portions of bowel resected. Continued below.
- For rectal cancers, determine and document the completeness of the mesorectal envelope:
- Complete: Specimen has intact mesorectum and peritoneal envelope all the way to the sigmo-rectal transition. The surface should be smooth and shiny with no exposed fat. There should be no “coning” of the envelope above the point of transection.
- Nearly complete: One or two areas of violation (~0.5 cm defects) of the mesorectal envelope with no loss of fat and no coning.
- Incomplete: Clear violation of mesorectal envelope with multiple areas of exposed fat and “coning in” at level of tumor.
- If not already done, photograph the mesorectal envelope (whether complete or incomplete).
- For colon tumors, palpate for tumor and ink the serosa adjacent to tumor. For rectal tumors (LAR, rectosigmoidectomy, APR), ink the radial margin. Also ink the mesenteric margin for non-rectal tumors (and for rectal tumors as well if the mesenteric margin is grossly identified). If unclear how to ink the specimen, please ask a PA.
- Open longitudinally along the anti-mesenteric border, unless this would mean cutting through the tumor.
- Take the following measurements:
- length of the colon (and ileum if present)
- circumference of bowel at the proximal and distal resection margins
- narrowest circumference at the tumor site
- wall thickness
- maximal tumor size in three dimensions
- distance of the tumor from the proximal and distal margins
- distance to mesenteric / radial margin
- note relationship of tumor to peritoneal reflection (above or below)
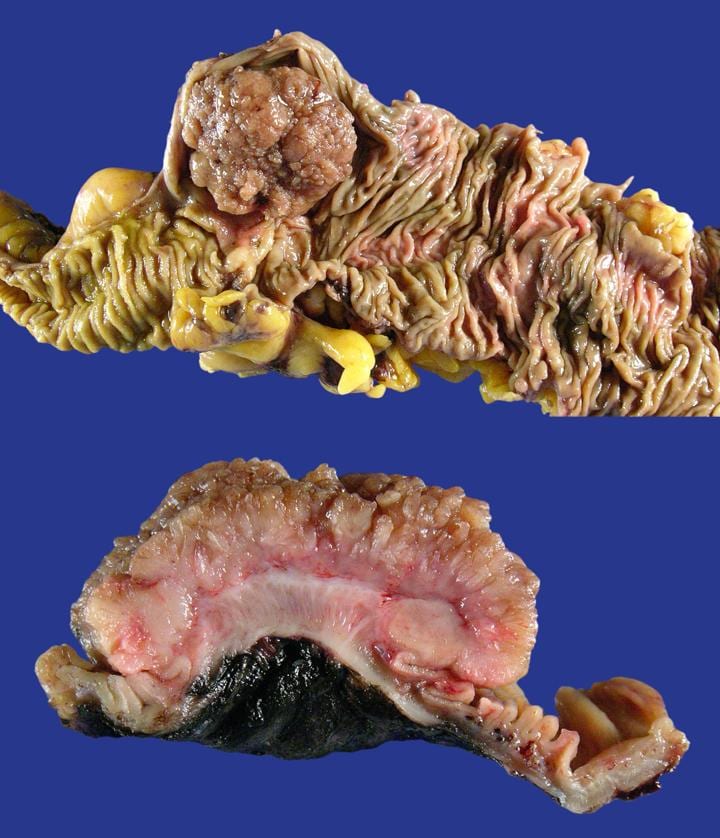
- Photograph
- Pin out on wax and fix in formalin overnight

Gross
- For oriented transanal mucosal resections, submit proximal and distal margins separately. Serially section and submit the remainder of the specimen. These sections will encompass lateral and deep margins.
- For larger resections, margins should be submitted as follows:
- Nearest Margin: If the tumor is within 2.0 cm of the nearest margin: ink the margin a different color, remove the proximal 2 cm of margin (with lesion and margin), section perpendicularly to the margin, and submit entirely (or showing closest approach to margin). If there is remaining margin grossly >2.0 cm from lesion, a representative section can be submitted en face. (see diagram)
- Farthest Margin: If the tumor is > 2.0 cm from one or both margins: submit either a) circumferential margin (if small diameter), b) a representative en face section, or c) a representative perpendicular section. (see diagram)

- Serially section tumor and measure depth of invasion into wall and distance from inked serosa. Identifying this accurately is key. The depth of invasion/T stage is important prognostic indicator.
- In APR/rectosigmoidectomy/LAR, identify and ink the radial margin (non-peritonealized surface). Measure the maximal fat thickness in this area. Measure the distance between tumor (or deepest ulceration) and ink. The radial margin assessment is an important prognostic indicator.
- Photograph cut surface at deepest point of invasion.
- Take at least three sections of the tumor, to include the maximal depth of invasion.
- If only treated TUMOR BED is present, submit ENTIRELY. However, if residual tumor is grossly evident, only REPRESENTATIVE SECTIONS focusing on the area of deepest invasion are needed.
- Shave and submit mesenteric margin if applicable (one cassette worth of tissue).
- Describe and submit any additional lesions and appendix if attached.
- Dissect and submit as many lymph nodes as you can find: Most of the nodes will be directly adjacent to the serosal surface of the colon. Nodes are rarely found in lobulated/mesenteric fat except along large vessels. Nodes are difficult to find below the peritoneal reflection in APR or LAR specimens. RULES OF THUMB:
- Submit ALL the lymph nodes you can find.
- If you cannot find adequate lymph nodes (at LEAST 14 are required for staging), ASK A PA for help.
- If neither you nor a PA can find any / adequate lymph nodes, submit at least ADDITIONAL 10 cassettes of fat, trimmed thinly.
- If adequate lymph nodes are not identified, you may need to go back to the bucket.

Updated 4/25/24 SRR, 9/12/24 NAC
