
Auto text: “Insert Thyroid Diffuse” or “Insert Thyroid Nodule”
For Demonstrative Video, click here!
As of 5-27-25: Inking of thyroid is updated per clinical request – please see below for differential inking of posterior surface:
Triage:
- Weigh
- Measure right lobe, left lobe, isthmus in 3 dimensions (S-I, M-L, A-P)
- Ink outer surface: Per clinical request, we are implementing new thyroid inking that differentially separates the anterior and posterior surfaces, in light of clinical differences in positive margins:
-
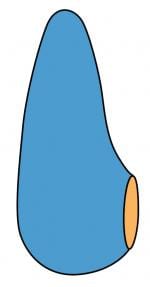
If the specimen is a lobectomy or hemithyroidectomy (lobe + isthmus):
-
- ink the ANTERIOR surface of the lobe and isthmus one color (BLUE or BLACK)
- ink the POSTERIOR surface RED
- ink the CUT surface of the lower lobe / isthmus ORANGE
-
- Please do this for ALL lobectomies, hemithyroidectomies, completion thyroidectomies, regardless of whether the opposite lobe is resected during the same procedure or not:
-
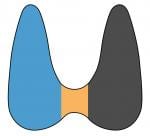
If the specimen is an intact total thyroidectomy with an appreciable isthmus:
- Ink the ANTERIOR surface of the LEFT lobe BLACK
- Ink the ANTERIOR surface of the RIGHT lobe BLUE
- Ink the ANTERIOR surface of the ISTHMUS ORANGE
- Ink the ENTIRE POSTERIOR surface RED
-
If the specimen is an intact total thyroidectomy with NO appreciable isthmus, you can eliminate orange:
- Ink the ANTERIOR surface of the LEFT lobe BLACK
- Ink the ANTERIOR surface of the RIGHT lobe BLUE
- Ink the ENTIRE POSTERIOR surface RED

- Fix in formalin overnight (Fix ALL thyroids! This procedure may help eliminate artifactual nuclear atypia and architectural distortion.)

Gross:
- Check for a possible central lymph node packet at the inferior poles, often near the isthmus. You should submit any possible lymph nodes as you normally would for a neck dissection, giving the count and size.
- Check ultrasound and FNA reports for number/location of nodules and cytologic diagnoses. This clinical information will help guide your dissection.
- How to serially section: Consider the TRANSVERSE approach versus the MODIFIED TRANSVERSE VERTICAL approach:
- An entirely TRANSVERSE approach should be used in most cases (multinodular disease with no dominant nodule, diffuse medical disease (Graves, Hashimoto), or a malignant diagnosis on FNA).
- The MODIFIED TRANSVERSE VERTICAL approach should be considered when there is a dominant nodule (indeterminate on FNA) of approximately 2 cm or larger. This method allows for visualization of the “tips” of the nodule within the lobe and facilitates subsequent sectioning perpendicular to the superior and inferior tips.
- TRANSVERSE METHOD:
- If the specimen is a lobectomy or hemithyroidectomy (lobe + isthmus): Each lobe should be serially sectioned transversely from superior to inferior (i.e. perpendicular to the long axis). Include isthmic orange margins in your transverse sections.

- If the specimen is an intact total thyroidectomy with an appreciable isthmus, the lobes should be sectioned transversely and the isthmus should be sectioned sagittally (from right to left or vice versa).
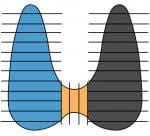
- If the specimen is an intact total thyroidectomy and the isthmus is short/inconspicuous, the lobes should be sectioned transversely, and isthmus can be included in your right and left lobe sections.

- MODIFIED TRANSVERSE VERTICAL METHOD:
- Please feel free to reach out to Dr. Cipriani if you are considering this method but are unsure of its utility.
- This method should be used for follicular neoplasms (NOT papillary or medullary carcinoma) in order to better visualize the location of the nodule, in order to facilitate perpendicular sectioning of the TIPS of the NODULE.
- The lobe should be bisected longitudinally (usually in the coronal plane) to expose the lesion, as such:
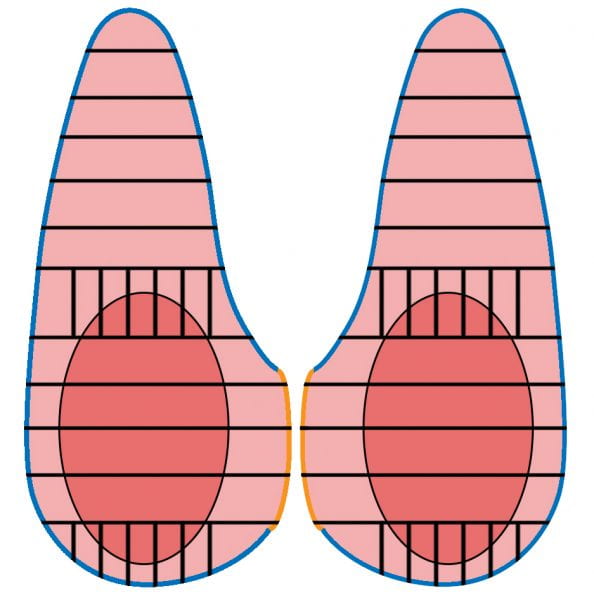
- The tips or ends of the nodule should then be sectioned perpendicularly in order to better visualize the interface of tumor with capsule on the microscopic slides.
- The center of the nodule and the remainder of the uninvolved thyroid can be sectioned in the standard transverse/axial plane.
- Please PHOTOGRAPH at least one of the bisected halves.

QUICK TIP: For Lobes/Hemis <10 g or Totals < 20 g, you can submit the entire specimen sequentially. Otherwise, follow guidelines below:
- For thyroids with 1) no nodules or 2) multiple coalescent nodules without a dominant or clinically suspicious nodule:
- Quick text is: “insert thyroid diffuse”
- Submit one cassette each of: right upper, right mid, right lower, left upper, left mid, left lower, isthmus
- You can put 1-2 sections in each cassette
- Submit all candidate lymph nodes and parathyroids (these are usually located at the isthmus)
- For thyroids with 1) single dominant nodule or 2) multiple clinically suspicious nodules:
- Quick text is “insert thyroid nodule”
- Document the location and size of nodules.
- PHOTOGRAPH cut sections of relevant / dominant nodule(s).
- If lesion is grossly infiltrative or has an undulating or ill-defined edge: Submit representative sections, at least 1 per cm, including nearest margin and interface with normal.
- If lesion is well-circumscribed (encapsulated or unencapsulated): Submit representative full sections of tumor AND a few additional cassettes of the interface with normal (multiple strips per cassette). If you think the lesion may have a CAPSULE, photograph a representative cross section. You do not necessarily need to submit the entire periphery of the lesion up front. If we determine histologically that there is a true capsule, we can always submit more.
- Document in your gross description whether extrathyroidal extension into fat, skeletal muscle, or other anatomic landmarks is visible.
- Submit other suspicious/discrete lesions
- Submit representative uninvolved normal, documenting location in your cassette summary: RUL, RML, RLL, LUL, LML, LLL, Isthmus
- Submit all candidate lymph nodes and parathyroids
- For Medullary Carcinoma or MEN syndrome patients:
- If the patient is undergoing prophylactic thyroidectomy for MEN syndrome, submit the entire thyroid sequentially.
- If the patient already has known medullary carcinoma, submit at least one extra cassette each of bilateral upper-mid poles (to assess for C-cell hyperplasia).
- You can put 1-2 sections in each cassette.
- For other cancer syndrome patients (DICER, PTEN):
- Submit the entire thyroid sequentially.
Updated 2-14-19, 4-14-22, 5-23-25 NAC.
